Patients with suspected ACS should be risk stratified based on the likelihood of ACS and adverse outcome(s) to decide on the need for hospitalization and assist in the selection of treatment options.
I
B
Emergency Department or Outpatient Facility Presentation
Recommendations
Class
Level
Patients with suspected ACS and high-risk features such as continuing chest pain, severe dyspnea, syncope/presyncope, or palpitations should be referred immediately to the ED and transported by emergency medical services when available.
I
C
Patients with less severe symptoms may be considered for referral to the ED, a chest pain unit, or a facility capable of performing adequate evaluation depending on clinical circumstances.
IIb
C
Prognosis: Early Risk Stratification
Recommendations
Class
Level
In patients with chest pain or other symptoms suggestive of ACS, a 12-lead ECG should be performed and evaluated for ischemic changes within 10 minutes of the patient’s arrival at an emergency facility.
I
C
If the initial ECG is not diagnostic but the patient remains symptomatic and there is a high clinical suspicion for ACS, serial ECGs (e.g., 15- to 30-minute intervals during the first hour) should be performed to detect ischemic changes.
I
C
Serial cardiac troponin I or T levels (when a contemporary assay is used) should be obtained at presentation and 3 to 6 hours after symptom onset all patients who present with symptoms consistent with ACS to identify a rising and/or falling pattern of values.
I
A
Additional troponin levels should be obtained beyond 6 hours after symptom onset in patients with normal troponin levels on serial examination when changes on ECG and/or clinical presentation confer an intermediate or high index of suspicion for ACS.
I
A
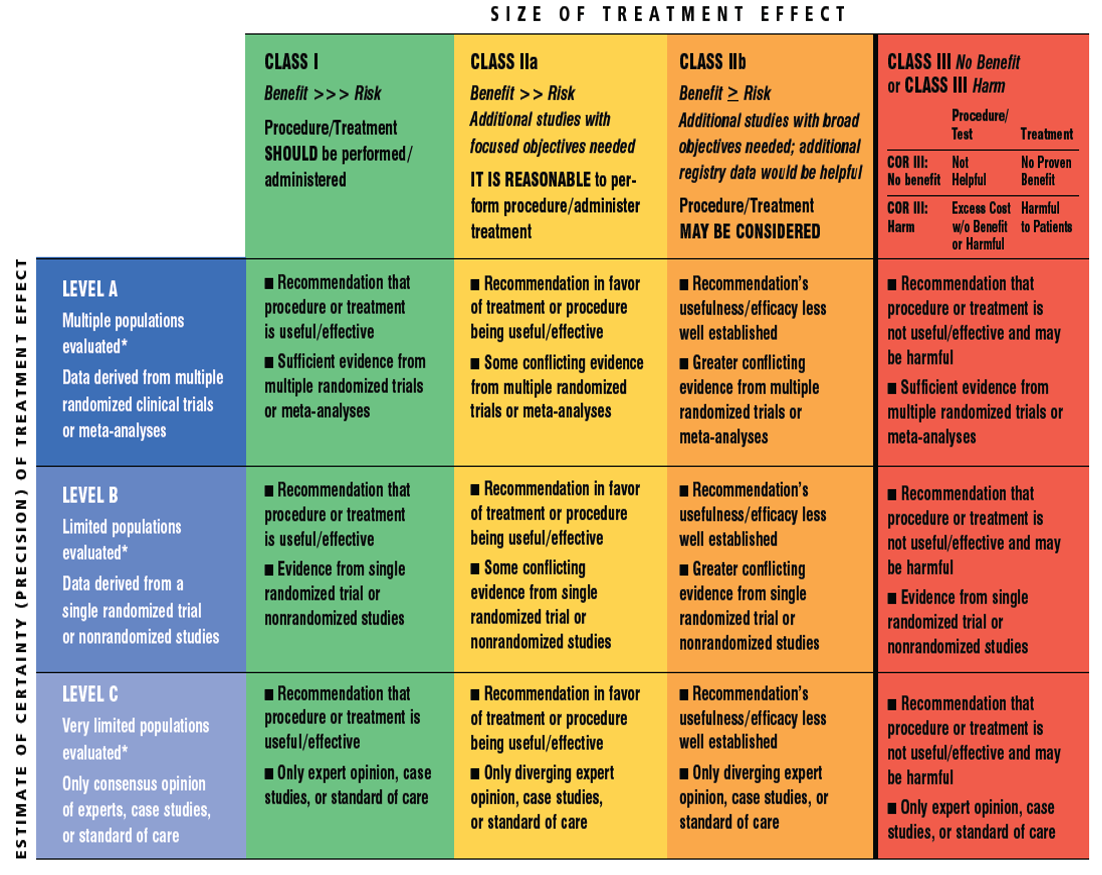
Risk scores should be used to assess prognosis in patients with NSTE-ACS.
I
A
Risk-stratification models can be useful in management: see below.
IIa
B
It is reasonable to obtain supplemental electrocardiographic leads V7 to V9 in patients whose initial ECG is nondiagnostic and who are at intermediate/high risk of ACS.
IIa
B
Continuous monitoring with 12-lead ECG may be a reasonable alternative in patients whose initial ECG is nondiagnostic and who are at intermediate/high risk of ACS.
IIb
B
Measurement of B-type natriuretic peptide or N-terminal pro–B-type natriuretic peptide may be considered to assess risk in patients with suspected ACS.
IIb
B
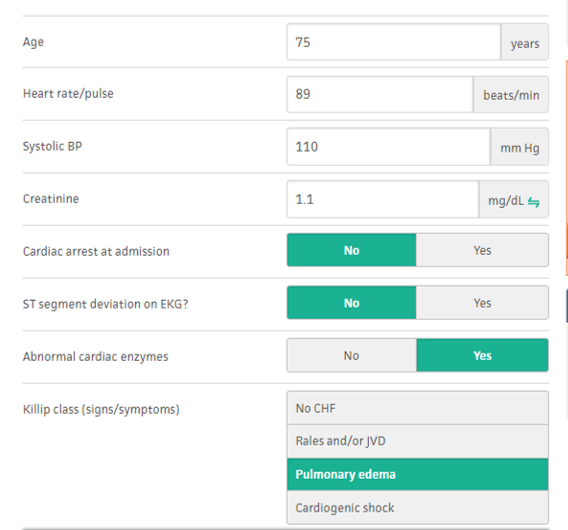
Risk: Thrombolysis in Myocardial Infarction (TIMI) Risk Score
TIMI Risk Score
All-Cause Mortality, New or Recurrent MI, or Severe Recurrent Ischemia Requiring Urgent Revascularization Through 14 d After Randomization, %
Cardiac-specific troponin (troponin I or T when a contemporary assay is used) levels should be measured at presentation and 3 to 6 hours after symptom onset in all patients who present with symptoms consistent with ACS to identify a rising and/or falling pattern.
I
A
Additional troponin levels should be obtained beyond 6 hours after symptom onset in patients with normal troponins on serial examination when electrocardiographic changes and/or clinical presentation confer an intermediate or high index of suspicion for ACS.
I
A
If the time of symptom onset is ambiguous, the time of presentation should be considered the time of onset for assessing troponin values.
I
A
With contemporary troponin assays, creatine kinase myocardial isoenzyme (CK-MB) and myoglobin are not useful for diagnosis of ACS.
III
A
Cardiac Biomarkers: Prognosis
Recommendations
Class
Level
The presence and magnitude of troponin elevations are useful for short- and long-term prognosis.
I
B
It may be reasonable to remeasure troponin once on day 3 or day 4 in patients with MI as an index of infarct size and dynamics of necrosis.
IIb
B
Use of selected newer biomarkers, especially B-type natriuretic peptide, may be reasonable to provide additional prognostic information.